

What Is A Nail Biopsy Fpr
one Department of Dermatology, Venereology and Leprology, University Higher of Medical Sciences, Delhi, Bharat
2 Section of Pathology, Maulana Azad Medical College, New Delhi, India
3 Department of Dermatology, Venereology, and Leprology, Mamata Medical College, Khammam, AP, India
Correspondence Accost:
Chander Grover
420 B, DDA Flats, Pocket Two, Mayur Vihar Phase I, Delhi 110 091
India
Introduction
The nail biopsy (NB) is a useful technique to obtain a diagnosis of a clinically cryptic blast status that is not diagnosable by history, clinical appearance and routine mycology. [one] Information technology is an investigation that not only provides etiologic, diagnostic and prognostic information merely too aids in understanding the pathogenesis of nail diseases. [2] No doubt information technology is of swell academic value, but the question addressed in this manuscript is the practical utility of NB in our day to day dermatologic practice. This article is not aimed at teaching the NB techniques in great detail but at putting forth applied tips, practise′due south and don′ts with respect to a NB.
For years, NB has been shunned as a difficult and scarring process, which is seldom required in solar day to day practice. [2] Just a few studies with a express number of patients have been carried out to appraise the utility of NB in dermatology, [2],[iii],[4],[5] while some others have focussed on histopathology of specific nail diseases, e.thou. onychomycosis, [6],[7] psoriasis, [4],[8] melanonychia, [nine],[x] etc. Apart from these attempts, NB and nail histopathology have not been in much vogue either in the literature or in exercise due to various factors. The objective of a NB is to arrive at a precise diagnosis of nail pathology with a simple, condom surgical procedure, simultaneously avoiding pain or permanent nail dystrophy. [one] Non every patient needs to undergo NB but, when required, there are certain essential prerequisites to be fulfilled.
Prerequisites for A Nail Biopsy
Knowledge of nail anatomy
A precise understanding of the nail anatomy is an essential prerequisite, and 1 can refer to standard texts on this subject every bit information technology is out of scope of the present communication. [1],[11] While operating, the boom unit beefcake should be thoroughly respected. The essential structures like the ventral and proximal nail matrix (responsible for nail plate surface), the distal smash matrix (responsible for nail plate structure and adherence to nail bed), and the extensor tendons (responsible for normal motion and function) of the digit should exist safeguarded. Because of the absence of any subcutaneous tissue in the nail unit of measurement, whatever biopsy of the nail unit needs to be taken downwards to the periosteum.
Patient selection
Patient choice is of import every bit NB needs to be performed only for a patient in whom the diagnosis has non been forthcoming due to the absence of typical skin lesions or histopathology and the nail status does non yield adequate information on routine investigations similar straight microscopy or culture. An ideal candidate for NB should be the one in whom either there are no skin lesions or they are not contributing towards a diagnosis, as skin biopsy is e'er a safer and easier procedure than NB. Patients with diabetes, peripheral vascular disease, or arterial insufficiency should not be subjected to NB. [12] An informed written consent should be taken every bit with all other surgical procedures.
Surgical technique
Exsanguination followed by a digital tourniquet is also an essential prerequisite for any fruitful process, as the nail bed is a highly vascular construction that may bleed profusely when manipulated. It is important to note that the tourniquet should non exist kept on for more than than 15 min at a stretch. [1] Commonly used nail unit of measurement anesthesia techniques include the proximal "band cake" (infiltration of anesthetic solution at the base of the digit) or the distal "fly block" (infiltration in the proximal and lateral nail folds). [ane]
Instrumentation
Appropriate instruments brand life like shooting fish in a barrel for any nail surgeon. The nail spatula/elevator, nail splitter, and sharp biopsy punches (3 mm and 4 mm) are accented must haves for a nail surgeon. Skin hook, fine-tipped, curved atraumatic forceps and pair of scissors are valuable add-ons [Figure - one].
 |
| Figure one: Instruments required for a nail biopsy. Shown are fine curved (Castro Veijo's) scissors, fine curved (Jeweller's) forceps, nail spatula, boom splitter, and disposable biopsy punches (3 mm and four mm) |
Histopathology
A competent dermatopathologist who is familiar with the bones histopathologic features of the nail is also an essential prerequisite. It is of import to note that there are basic differences in nail histopathology in wellness as well every bit in affliction, as compared to that of the peel, and these need to be understood and appreciated. [13] Proper embedding and sectioning of the NB specimen is essential prior to this.
Side-effects
The risks associated with the NB procedure should be explained and consent of the patient must be obtained beforehand. These include the possibility of permanent nail dystrophy, possibility of non achieving a diagnosis even after NB, more time required for regrowth of the nail, bleeding, and take chances of infection as with any other surgery.
Techniques/Types
NB could be taken equally an excision biopsy, punch biopsy, or longitudinal biopsy. A punch or an excision biopsy can be applied to any individual anatomical part of the nail unit of measurement, like the nail bed, nail plate, boom fold, or matrix. A longitudinal NB gives maximum histopathological data, but it is not routinely resorted to due to its scarring potential. Nail as a unit is capable of producing a very express set of clinical reaction patterns, eastward.g. onycholysis tin can be a manifestation of onychomycosis, blast psoriasis, or even boom lichen planus. Hence, finding a histopathologic cause is generally required prior to initiating specific therapy. The fob lies in choosing the area to be biopsied, i.e. the surface area that will bear witness the histopathological diagnostic changes, and [Table - 1] can serve as a guide in this regard. Every bit is well known, the changes in nail plate occur as a effect of the pathology of the smash matrix; hence, the histopathological features of disorders like melanonychia, erythronychia, pitting, etc. are best represented in a boom matrix biopsy. Even so, for features similar onycholysis, subungual hyperkeratosis, salmon patch, etc. 1 would need to have a nail bed biopsy.
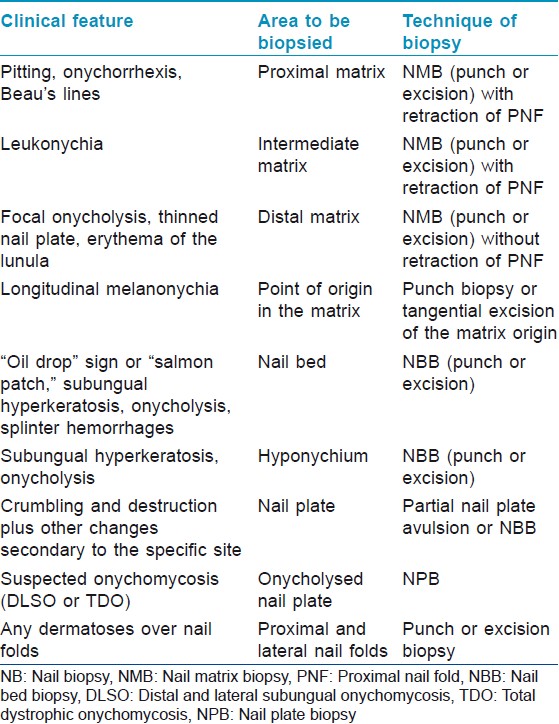
Tabular array 1: Site and technique of boom biopsy for mutual nail disorders
Based on the site from where it is being taken, NB tin can be classified as follows [Figure - 2]:
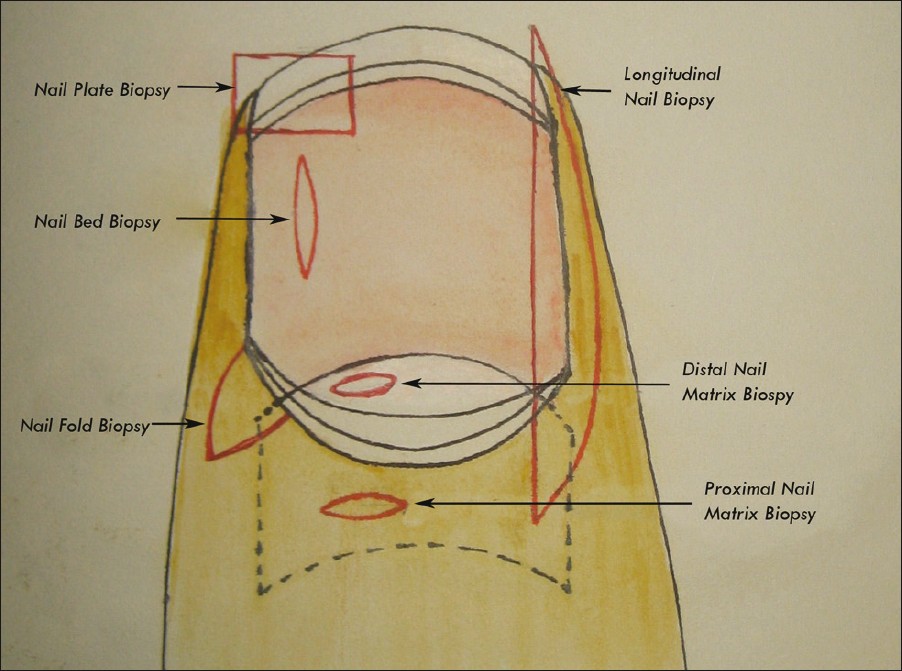 |
| Figure two: Different types of nail biopsy. The incision lines are shown in red |
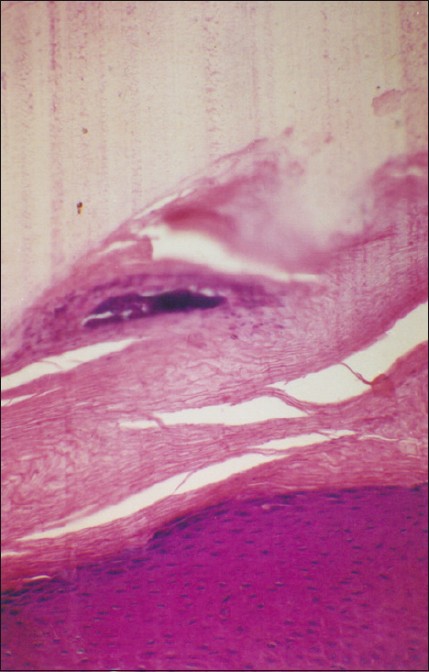
- Blast plate biopsy (NPB) is the easiest and the least-scarring technique, wherein a function of the nail plate (onycholysed or not) is separated and sent for histopathologic analysis. [7] It gives limited histopathological data but is useful in suspected cases of onychomycosis (demonstrates nail plate fungal invasion), [7] warts (adherent epithelium will show koilocytes [2] ) [Figure - 3], and also nail psoriasis (nail plate neutrophilic infiltration, serum crusts, and parakeratosis can be hands seen). The utility of NPB in systemic affliction has also been explored extensively. [14]
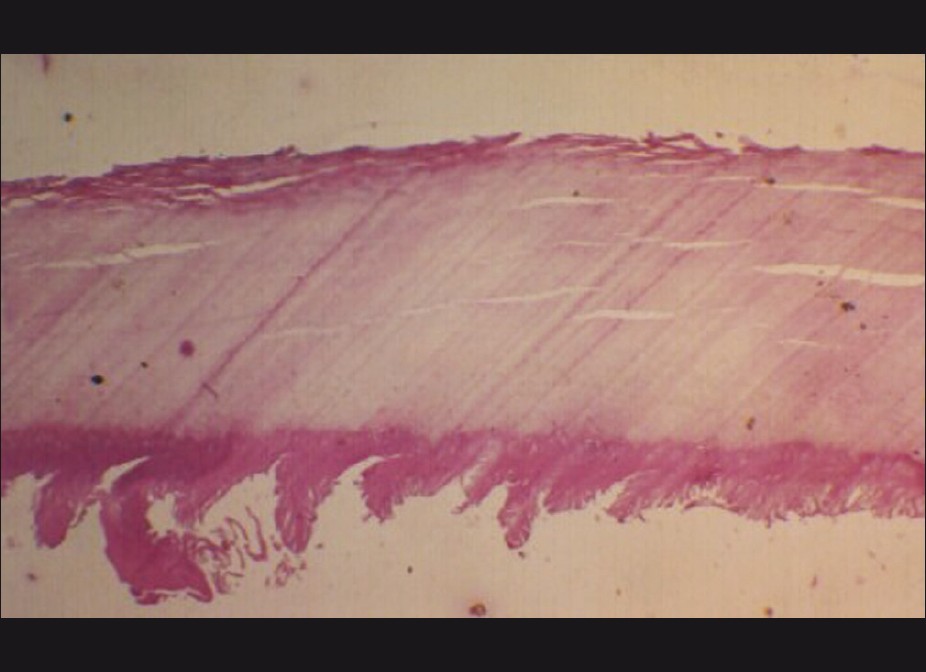
Figure iii: Nail plate biopsy with adherent smash plate epithelium showing bear witness of a subungual wart. Note the marked papillomatosis of the blast bed epithelium (H and E, ×60) - Nail bed biopsy (NBB) is generally performed to distinguish between two or more conditions with a like clinical pattern, similar onycholysis or subungual hyperkeratosis, cases with discoloration of the nail bed, or any painful nail bed lesion. It can be an elliptical excision (longitudinally oriented) or a dial biopsy [Figure - 4]. Prior nail avulsion may or may not be required. If required, and then fractional avulsion to expose the surface area to be biopsied is preferred to full avulsion. Nail bed defects upwards to 3 mm can be left unsutured. [1],[12] Postoperative healing of the nail bed is generally uneventful, and the incidence of scarring and onycholysis is low. NBB is of therapeutic utility in cases with nail bed tumors, like glomus tumor.

Effigy 4: Procedure of a smash bed biopsy. (a) Suspected blast bed glomus tumor. (b) Subungual glomus tumor seen equally a bluish mass after nail plate avulsion. (c) Excision of the tumor done. Note that the nail bed incisions are oriented longitudinally. (d) Defect >3 mm in width needs to exist sutured - Blast fold biopsy (NFB) can exist done from the proximal (PNF) or lateral nail fold (LNF), and is indicated for paronychial dermatoses, inflammation, or nail fold tumors (beneficial or malignant). It tin be shave biopsy, elliptical excision, punch, or en bloc excision (for PNF). [15] Prior to any excision over the nail folds, it is wise to insert a nail spatula underneath the concerned fold to prevent any inadvertent damage to the underlying blast bed or matrix.
- Nail matrix biopsy (NMB) is resorted to for the exploration of matrix origin of longitudinal pigmented bands, benign lesions of the boom matrix (glomus tumor), malignant lesions (melanoma), or caused smash plate defects similar punctate leukonychia, onychorrhexis, or pitting. The techniques employed are elliptical excision (horizontally oriented), dial excision (≤3 mm), and tangential (shave) excision. A proximal blast fold-lunula double-punch technique has also been described. [sixteen] Whenever possible, the distal matrix should be biopsied rather than the proximal matrix, and the lunular margin should non be compromised to minimize scarring. If a biopsy is to be taken from the proximal matrix, lateral release incisions at the junction of proximal and lateral nail folds forth with stay sutures (every bit shown) aid in exposing the proximal matrix area [Figure - 5].

Figure five: Procedure of nail matrix biopsy. For adequate exposure of the proximal matrix, lateral incisions are made at the junction of the proximal and lateral nail folds. The proximal blast fold is then lifted up and retracted with the help of stay sutures. An adequate - sized punch is and then driven downwardly up to the periosteum and the punch biopsy specimen is lifted up - Longitudinal nail biopsy (LNB) is performed when it is desirable to sample the unabridged nail unit of measurement. [17],[xviii] The resultant defect needs to be sutured to ensure proper healing [Figure - 6]. It is a very useful technique for the treatment of larger lesions placed asymmetrically over the afflicted nail. This technique samples the representative areas of each function of the nail unit, and has been of immense bookish aid. Even so, being a potentially scarring procedure, its utility in day to day clinical do is low.

Effigy 6: Procedure of longitudinal nail biopsy. (a) The area to exist excised is outlined. The incision is linear medially and curved laterally. (b) The incision is carried down to the periosteum and the tissue is lifted up with sharp dissection. (c) The separated specimen for histopathologic examination. (d) The defect is sutured back
Boom plate specimens when taken as a function of biopsy need to be softened before processing. For this purpose, various agents have been recommended, which include 3% phenol, cedar wood oil, and chitin-softening solutions composed of mercuric chloride, chromic acid, acetic acrid, and 95% alcohol. [two]
Complications expected with the NB include bleeding, secondary infection, scarring of nail bed, onycholysis, and reduction in nail width, malalignment of the centrality of the regrowing blast, or growth of nail spicules. [12] The terminal 3 are almost exclusively seen with LNB .
Histopathology
The blast unit of measurement has few histopathological features distinct from the normal skin [thirteen] [Figure - seven]. Smash fold epithelium lacks any pilosebaceous units, and rete ridges are also minimal to absent-minded. Blast matrix epithelium has wide, lodge-shaped rete ridges pointing proximally. It is devoid of a granular layer and undergoes onychokeratinisation to produce the nail plate. In that location is a high density of melanocytes seen even in layers above the basal layer. Nail plate is composed of cornified cells without nuclei, arranged in lamellae that stain strongly with acid fast stains. Nail bed epithelium is only two to iii layers thick, devoid of a granular layer, and lacks rete ridges in a sagittal department. The granular layer reappears in the epithelium of the hyponychium. The dermis is highly vascular, containing numerous nerve endings, specialized nerve structures, and glomus bodies.
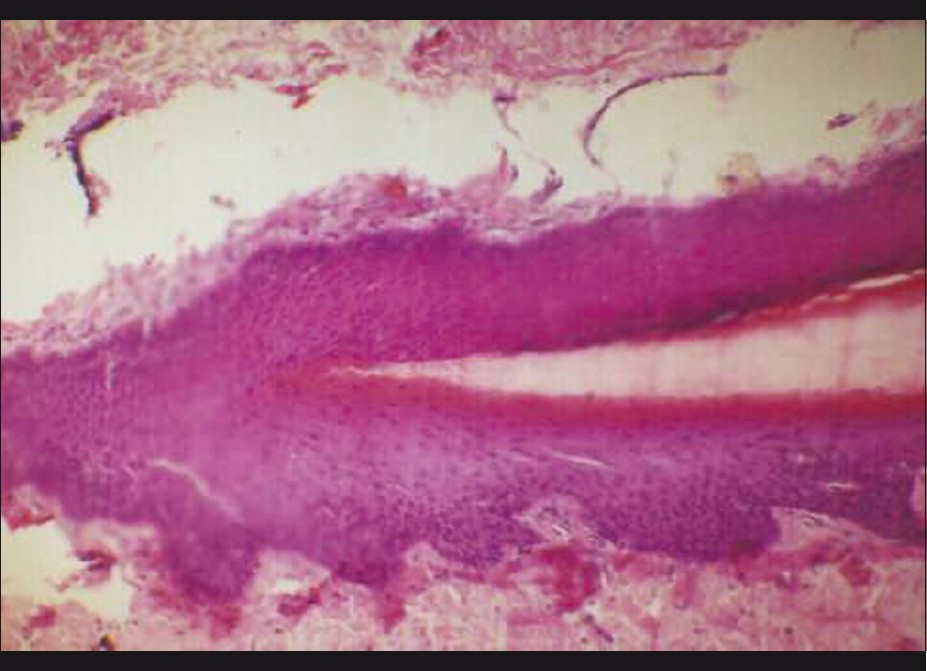 |
| Figure 7: Normal smash unit histopathology showing the blast matrix area. The nail plate is seen arising over the nail matrix expanse. The feature absence of granular layer in the boom matrix epithelium can exist noted (H and East, ×160) |
Not surprisingly, the nail unit histopathology features in disease are also quite different, e.thousand. in dissimilarity to skin psoriasis, smash psoriasis is characterized by hypergranulosis. The salient features of smash histopathology in selected diseases are outlined in [Tabular array - 2]. [2],[iv],[xiii] One fact to be borne in mind is that the thin nail bed epithelium is tightly adherent to the blast plate and tends to get avulsed forth with it. Hence, a NBB performed after avulsing the blast plate may non requite adequate histopathological information, especially in case of inflammatory nail pathology (personal ascertainment) [Figure - 3].
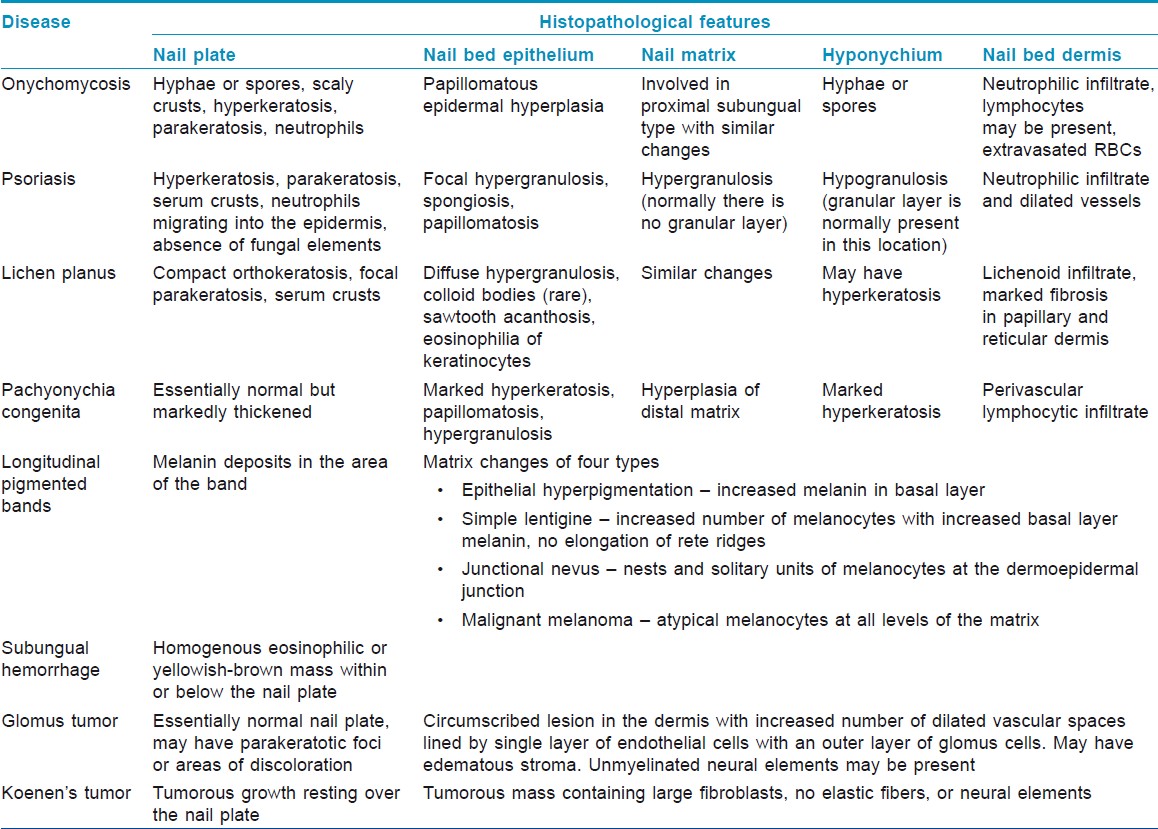
Table ii: Salient histopathological features of common blast disorders
Indications
Earlier studies have described varying degrees of success in establishing a diagnosis with NB. Hanno et al. studied predominantly inflammatory blast pathologies and found diagnostic features in xl% of their cases. [4] In the series past de Berker et al. comprising mainly of tumors, 93.93% biopsies were diagnostic. [5] Grover et al. evaluated sixty blast biopsies of infective too every bit noninfective disorders, and found diagnostic histopathology in 64% cases. [ii] NB was reported especially useful for definitive diagnosis in blast tumors and infections. [ii],[4],[v] All these studies accept documented a depression risk of side-effects to NB and demonstrated it to be a elementary and safe procedure. [2],[7],[12] A skillfully performed adequate NB, handled, processed, and interpreted properly, can be an of import part of the dermatologist′s armamentarium in providing excellent, comprehensive patient intendance. [19]
The utility of diverse types of NB has been studied extensively for various common and uncommon boom disorders.
Onychomycosis
This has been an area of active inquiry, [vi],[7],[20],[21] and NB with PAS staining has been reported to be the nearly sensitive method for diagnosis [half-dozen] [Figure - 8]. Routine histological examination with PAS staining before initiating antifungal therapy was recommended initially. [21] However, in later studies, histopathologic exam has been proposed as a useful costless test, indicated if results of other methods are negative and clinical suspicion is loftier. [6],[7]
 |
| Figure 8: Fungal pseudohyphae seen in a nail plate biopsy (H and East, ×400) |
Twenty smash dystrophy
NB has revealed that the disorder Xx nail dystrophy (TND) is multifactorial in origin as it may show histopathologic features of nail psoriasis, lichen planus, or spongisosis. [18],[22],[23],[24] NB has a definite diagnostic utility in cases with TND, where the clinical diagnosis is obscure because of the absence of cutaneous associations. However, it cannot be recommended for the routine evaluation of this otherwise benign disorder, especially because the further treatment options are generally not altered. [25]
Blast psoriasis
NB for blast psoriasis has been an expanse of involvement, especially because 1-5% of the cases with psoriasis may present with purely nail manifestations only. [8] Hanno et al. proposed diagnostic criteria of nail psoriasis in the form of presence of neutrophils in the nail bed epithelium (major benchmark), hyperkeratosis with parakeratosis, serum exudates, focal hypergranulosis, and nail bed epithelium hyperplasia (small-scale criteria) [4] [Figure - ix]. As onychomycosis may testify similar features, Grover et al. suggested that PAS negativity for fungal hyphae should be included every bit a major criterion for the diagnosis of smash psoriasis. [eight]
 |
| Figure 9: Nail unit biopsy showing psoriasis. Hypergranulosis, parakeratosis, parakeratotic abscess, and serum crusting can be appreciated (H and E, ×160) |
Nail lichen planus
Isolated boom lichen planus (LP) comprises 1-ten% cases of LP. As boom LP is potentially scarring and the changes may be irreversible, an effective direction of the condition requires that the diagnosis be confirmed on histopathology. The diagnostic features of boom LP accept been described on NB. [4],[26],[27] Peluso et al. reported the utility of NB in confirming the diagnosis of LP in an 11-yr-old male child, which enabled successful handling of the example [27] [Figure - 10].
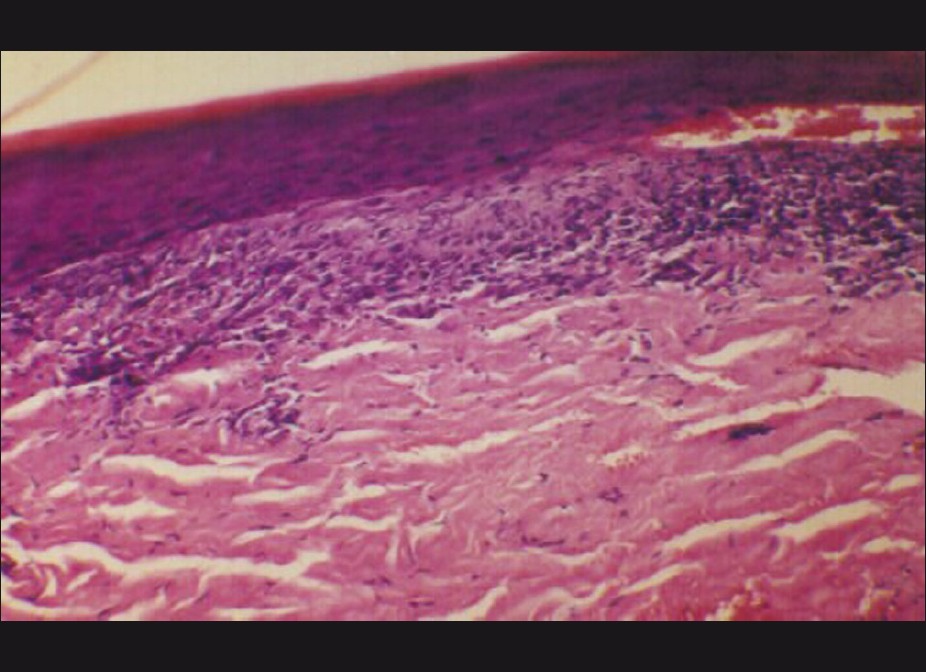 |
| Figure 10: Nail bed epithelium showing changes suggestive of lichen planus. Basal layer dissolution and a band-similar infiltrate hugging the epidermis tin exist seen (H and E, ×160) |
Other dermatoses
NB has been useful in establishing diagnosis in isolated nail lichen striatus [28] and sarcoidosis. [29] However, in PRP, the nail histopathological changes represent a nonspecific reaction design and are not diagnostic. [xxx] The ultrastructural studies of NPB have likewise been reported to be a useful diagnostic tool in distinguishing lamellar ichthyosis from other ichthyoses, with overlapping clinical features. [31]
Melanonychia
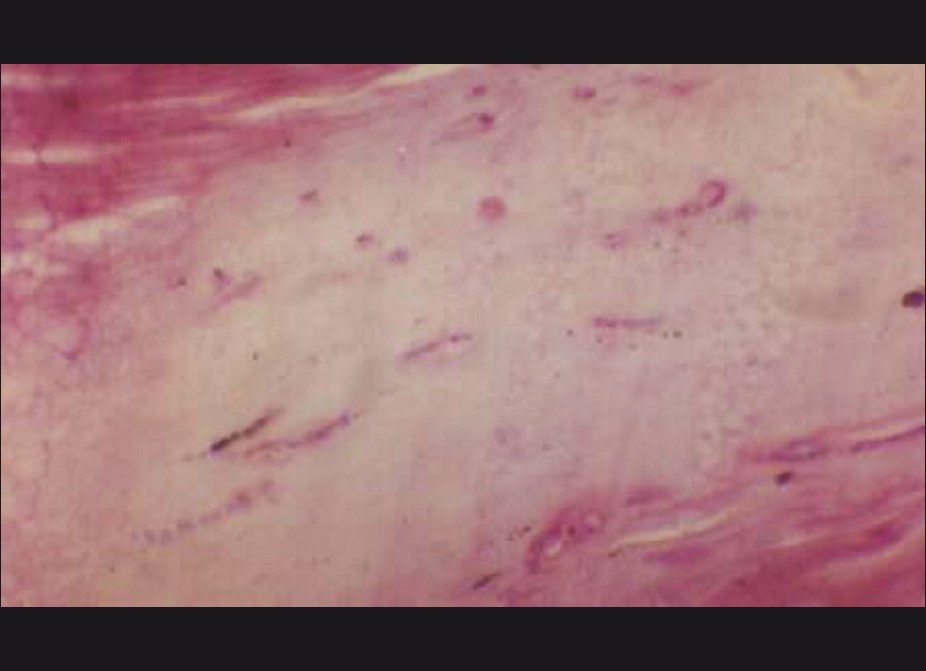
NB is of particular utilise in the evaluation of pigmented nails, specially longitudinal melanonychia. [nine],[10] Histopathologically, the matrix lesion responsible for pigmented nail bands may be of iv types [9] [Table - 2]. Epidermal hyperpigmentation represents melanocyte activation due to inflammation, trauma, friction, or drugs [Figure - xi]. Boom matrix may also have a simple lentigene or boom matrix nevus. However, the most ominous diagnosis is that of a malignant melanoma that can be effectively ruled out with a NB. Tosti et al. studied nail matrix nevi histologically in 22 patients and reported that a diagnosis of nail matrix nevus is impossible clinically and always requires histopathologic study. Further, blast matrix nevi resemble pare nevi histopathologically except for their architectural design, which reflects the peculiar beefcake of the nail unit of measurement. [ix]
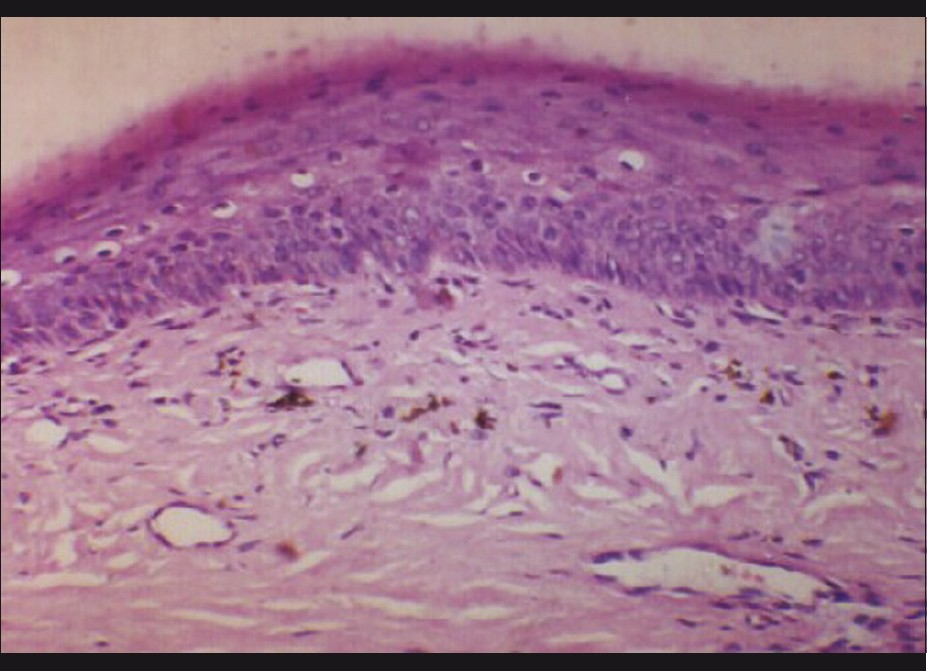 |
| Figure 11: Nail matrix biopsy from the case shown in Effigy 5, showing paint - laden cells in dermis-melanocyte activation (H and Due east, ×250) |
Tumors
Nail matrix is the nigh common site for Glomus tumor, and excision biopsy provides treatment, relief from pain, and histological diagnosis in 1 go [32] [Figure - four]. Periungual fibromas are benign tumors that are a cutaneous manifestation of tuberous sclerosis complex. They tin drain, cause pain, and distort the nail. Their histopathologic features have been studied in detail by Ma et al. [33] Squamous cell carcinoma is the other malignancy common in the nail bed that can be diagnosed hands with a NB. [34],[35]
Systemic diseases
NB (particularly NPB) has as well been reported to be useful in the written report of systemic diseases. Tirado-Gonzalez et al. proposed that fluids exude or transude into nail structures providing a kind of ′′smash window′′ into systemic hematologic or metabolic abnormalities. [14] Detection of urate crystals in the subungual horn of nails submitted for a suspected diagnosis of onychomycosis has been reported. [fourteen] It is even proposed that gout may be monitored past means of the uncomplicated and noninvasive histological processing of nail clippings. All the same, for proper evaluation of the character of such crystals, nail plate specimens need to exist submitted in booze rather than in formaldehyde. The presence of characteristic cytologic and histologic findings in a nail plate biopsy tin expand the armamentarium of physicians to evaluate nail diseases and even systemic diseases in a noninvasive style. [14] Bolliger et al. determined the urea, ammonia, and uric acrid content of toenails in 11 patients with varying types and degrees of renal impairment and found a markedly elevated content of uric acid in patients with chronic nephritis and with long-standing severe gout. [36]
Pros and Cons of Boom Biopsy
From the aforementioned discussion, information technology is clear that NB offers sure special advantages. NB, especially NPB, is a relatively easy procedure, to the lowest degree traumatic, and can be done hands. Information technology is seldom scarring except for the more radical LNB, which, anyhow, is non routinely resorted to by virtually of the dermatologists. NB is of utmost value in cases where no cutaneous changes are present, east.g. isolated boom psoriasis or nail lichen planus or other isolated nail dystrophies due to obscure dermatoses as described earlier. Hence, all of us demand to train ourselves to be able to perform NB and reach a conclusion rather than initiating therapy on the ground of conjectures [Table - 3].
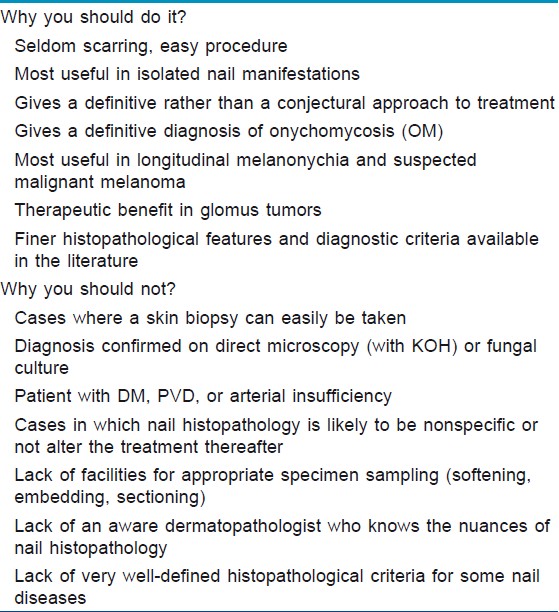
Tabular array 3: Pros and cons of a smash biopsy
NB provides a definitive diagnosis in onychomycosis every bit it reveals conclusive bear witness of nail plate invasion past the fungus, besides finer differentiating the cases with secondary contagion of subungual droppings of dystrophic nails. The conventional techniques of direct microscopy and civilisation for mycotic elements may requite a faux-positive report in such cases, due to which unnecessary and unsuccessful handling may be resorted to. NB is also the single most sensitive technique of these 3 procedures. [6] In addition, an expert dermatopathologist can besides differentiate between dermatophytes and NDM on routine histopathology thus giving valuable data regarding the choice of appropriate drug. [37] Poor growth rates on fungal civilization means that this information is generally non available to the treating dermatologist.
In cases with melanonychia, NB is the merely investigation that tin give whatever answers, especially when melanoma is suspected. Excision NBB is of therapeutic do good in nail tumors, specially the glomus tumor. In TND, NB is the only technique that tin guide toward the underlying condition responsible.
Nevertheless, there are certain inherent disadvantages as well. The procedure should non be attempted without a proper cognition of smash unit anatomy, especially the matrix area. Attention to surgical technique, including proper anesthesia, is a must for achieving desirable outcomes. Experience goes a long fashion in improving the diagnostic yield and minimizing the associated procedural side-effects. The run a risk of long-term boom scarring if surgical technique is not proper and the risk of secondary infection, especially in a tropical state like ours, is to be taken care of. Likewise, one should exist able to choose the representative area that will yield the best diagnostic data. An essential requirement is an efficient dermatopathologist well versed in the estimation of normal and abnormal blast histology every bit there are many differences as compared with the normal and abnormal skin histology. A properly processed sample with a softened boom plate enables cutting of adept sections under a microtome, minimizing any cutting artefacts.
Current knowledge about the histopathological details on nail specimens is limited, especially in relation to the uncommon blast disorders. The diagnostic criteria for some common diseases like nail psoriasis and lichen planus are constantly beingness improved upon. Mayhap, this could partly be due to the reluctance of dermatologists towards obtaining a NB for diagnostic purposes, thereby resulting in the scarcity of NB specimens reaching pathology laboratories and curtailing the feel of pathologists in the field of histological estimation of NB.
Conclusion
A NB is not indicated for each and every disorder manifesting in the boom unit. However, when it is indicated, it is often the only inkling left to achieve a diagnosis. Hence, a practicing dermatologist cannot afford to be unaware of or untrained in the technique of obtaining NB. Further, pathologists need to exist trained in interpreting nail specimens, every bit the histopathological effect can only be improved with more familiarity, assessment of specimens, and refinement of diagnostic criteria. The more the specimens are seen, the more than details and refinements will emerge. With increased detailing, proper orientation and sectioning, sophisticated microtomes, and staining procedures, a wealth of information awaits u.s.a. in the humble nail.
References
| ane. | Rich P. Blast biopsy: Indications and methods. Dermatol Surg 2001;27:229-34. [Google Scholar] |
| ii. | Grover C, Nanda Due south, Reddy BS, Chaturvedi KU. Blast biopsy: Assessment of indications and issue. Dermatol Surg 2005;31:190-four. [Google Scholar] |
| three. | Barrera-Vigo MV, Tejera-Vaquerizo A, Mendiola-Fernández M, Cid J, Cabra-de Luna B, Herrera-Ceballos E. Diagnostic utility of nail biopsy: A study of 15 cases. Actas Dermosifiliogr 2008;99:621-seven. [Google Scholar] |
| 4. | Hanno R, Mathes BM, Krull EA. Longitudinal boom biopsy in evaluation of acquired nail dystrophies. J Am Acad Dermatol 1986;14:803-9. [Google Scholar] |
| five. | de Berker DA, Dahl MG, Comaish JS, Lawrence CM. Nail surgery: An assessment of indications and effect. Acta Derm Venereol 1996;76:484-7. [Google Scholar] |
| 6. | Weinberg JM, Koestenblatt EK, Jennings MB. Utility of histopathologic analysis in the evaluation of onychomycosis. J Am Podiatr Med Assoc 2005;95:258-63. [Google Scholar] |
| vii. | Grover C, Reddy BS, Chaturvedi KU. Onychomycosis and the diagnostic significance of nail biopsy. J Dermatol 2003;30:116-22. [Google Scholar] |
| 8. | Grover C, Reddy BS, Uma Chaturvedi Yard. Diagnosis of nail psoriasis: Importance of biopsy and histopathology. Br J Dermatol 2005;153:1153-viii. [Google Scholar] |
| 9. | Tosti A, Baran R, Piraccini BM, Cameli North, Fanti PA. Nail matrix nevi: A clinical and histopathologic study of 20-ii patients. J Am Acad Dermatol 1996;34:765-71. [Google Scholar] |
| 10. | Goettmann-Bonvallot Due south, André J, Belaich S. Longitudinal melanonychia in children: A clinical and histopathologic study of twoscore cases. J Am Acad Dermatol 1999;41:17-22. [Google Scholar] |
| 11. | deBerker DA, Baran R, Dawber RP. Disorders of nails. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology. 7 th ed, Massachusetts: Blackwell Publishing; 2004. p 62.1-viii. thursday ed, Massachusetts: Blackwell Publishing; 2004. p 62.1-8.'>[Google Scholar] |
| 12. | Moossavi One thousand, Scher RK. Complications of nail surgery: A review of the literature. Dermatol Surg 2001;27:225-8. [Google Scholar] |
| 13. | Jerasutus Due south. Histopathology. In: Scher RK, Daniel CR 3 rd , editors. Nails: Diagnosis, therapy, surgery. three rd ed, Philadelphia: Elsevier Saunders; 2005. P. 37-70. [Google Scholar] |
| 14. | Tirado-González M, González-Serva A. The smash plate biopsy may pick upwards gout crystals and other crystals. Am J Dermatopathol 2011;33:351-three. [Google Scholar] |
| 15. | Grover C, Bansal S, Nanda S, Reddy BS, Kumar V. En bloc excision of proximal blast fold for treatment of chronic paronychia. Dermatol Surg 2006;32:393-eight; discussion 398-nine. [Google Scholar] |
| sixteen. | Kim JE, Ahn HS, Cheon MS, Lee KJ, Cho BK, Park HJ. Proximal smash fold-lunula double dial technique: A less invasive method for sampling blast matrix without nail avulsion. Indian J Dermatol Venereol Leprol 2011;77:346-8. [Google Scholar] |
| 17. | Zaias N. The longitudinal nail biopsy. J Invest Dermatol 1967;49:406-eight. [Google Scholar] |
| 18. | Grover C, Khandpur S, Reddy BS, Chaturvedi KU. Longitudinal smash biopsy: Utility in 20-nail dystrophy. Dermatol Surg 2003;29:1125-9. [Google Scholar] |
| 19. | Fleckman P, Omura EF. Histopathology of the blast. Adv Dermatol 2001;17:385-406. [Google Scholar] |
| xx. | Scher RK, Ackerman AB. Subtle clues to diagnosis from biopsies of nails: The value of nail biopsy for demonstrating fungi not demonstrable by microbiologic techniques. Am J Dermatopathol 1980;2:55-7. [Google Scholar] |
| 21. | Machler BC, Kirsner RS, Elgart GW. Routine histologic exam for the diagnosis of onychomycosis: An evaluation of sensitivity and specificity. Cutis 1998;61:217-9. [Google Scholar] |
| 22. | Tosti A, Bardazzi F, Piraccini BM, Fanti PA. Idiopathic trachyonychia (twenty-nail dystrophy): A pathological study of 23 patients. Br J Dermatol 1994;131:866-72. [Google Scholar] |
| 23. | Tosti A, Fanti PA, Morelli R, Bardazzi F. Trachyonychia associated with alopecia areata: A clinical and pathologic study. J Am Acad Dermatol 1991;25:266-lxx. [Google Scholar] |
| 24. | Taniguchi Due south, Kutsuna H, Tani Y, Kawahira K, Hamada T. Xx-nail dystrophy (trachyonychia) caused past lichen planus in a patient with alopecia universalis and ichthyosis vulgaris. J Am Acad Dermatol 1995;33:903-5. [Google Scholar] |
| 25. | Grover C, Bansal S, Nanda Southward, Reddy BS. Efficacy of triamcinolone acetonide in various acquired boom dystrophies. J Dermatol 2005;32:963-8. [Google Scholar] |
| 26. | Tosti A, Piraccini BM, Cambiaghi S, Jorizzo M. Smash lichen planus in children: Clinical features, response to treatment, and long-term follow-upward. Arch Dermatol 2001;137:1027-32. [Google Scholar] |
| 27. | Peluso AM, Tosti A, Piraccini BM, Cameli N. Lichen planus limited to the nails in childhood: Case study and literature review. Pediatr Dermatol 1993;x:36-9. [Google Scholar] |
| 28. | Tosti A, Peluso AM, Misciali C, Cameli N. Nail lichen striatus: Clinical features and long-term follow-up of 5 patients. J Am Acad Dermatol 1997;36:908-13. [Google Scholar] |
| 29. | Mann RJ, Allen BR. Blast dystrophy due to sarcoidosis. Br J Dermatol 1981;105:599-601. [Google Scholar] |
| 30. | Sonnex TS, Dawber RP, Zachary CB, Millard PR, Griffiths Advertising. The nails in adult blazon 1 pityriasis rubra pilaris: A comparison with Sézary syndrome and psoriasis. J Am Acad Dermatol 1986;15:956-60. [Google Scholar] |
| 31. | Rice RH, Crumrine D, Hohl D, Munro CS, Elias PM. Cross-linked envelopes in boom plate in lamellar ichthyosis. Br J Dermatol 2003;149:1050-4. [Google Scholar] |
| 32. | Cigna E, Palumbo F, De Santo L, Edoardo Zampieri A, Soda Thou. Short-scar surgical approach for the treatment of glomus tumor of the digit. J Cutan Med Surg 2011;15:21-8. [Google Scholar] |
| 33. | Ma D, Darling T, Moss J, Lee CC. Histologic variants of periungual fibromas in tuberous sclerosis circuitous. J Am Acad Dermatol 2011;64:442-4. [Google Scholar] |
| 34. | Dalle Due south, Depape L, Phan A, Balme B, Ronger-Savle S, Thomas 50. Squamous cell carcinoma of the nail apparatus: Clinicopathological study of 35 cases. Br J Dermatol 2007;156:871-4. [Google Scholar] |
| 35. | Gallouj S, Harmouch T, Soughi M, Baybay H, Meziane K, Hammas Northward, et al. Subungual verrucous carcinoma of the toe. Ann Dermatol Venereol 2010;137:842-iii. [Google Scholar] |
| 36. | Bolliger A, Gross R. Ammonia, urea and uric acrid content of toenails in renal insufficiency and gout. Aust J Exp Biol Med Sci 1953;31:385-xc. [Google Scholar] |
| 37. | Piérard GE, Arrese JE, De Doncker P, Piérard-Franchimont C. Nowadays and potential diagnostic techniques in onychomycosis. J Am Acad Dermatol 1996;34:273-7. [Google Scholar] |

Source: https://ijdvl.com/role-of-nail-biopsy-as-a-diagnostic-tool/
Posted by: alvaradobely1954.blogspot.com
0 Response to "What Is A Nail Biopsy Fpr"
Post a Comment